Boshoff, C.; Gray, B.
Article
The relationships between service quality, customer
satisfaction and buying intentions in the private
hospital industry
South African Journal of Business Management
Provided in Cooperation with:
University of Stellenbosch Business School (USB), Bellville, South Africa
Suggested Citation: Boshoff, C.; Gray, B. (2004) : The relationships between service quality, customer
satisfaction and buying intentions in the private hospital industry, South African Journal of Business
Management, ISSN 2078-5976, African Online Scientific Information Systems (AOSIS), Cape Town,
Vol. 35, Iss. 4, pp. 27-38,
https://doi.org/10.4102/sajbm.v35i4.666
This Version is available at:
https://hdl.handle.net/10419/218311
Standard-Nutzungsbedingungen:
Die Dokumente auf EconStor dürfen zu eigenen wissenschaftlichen
Zwecken und zum Privatgebrauch gespeichert und kopiert werden.
Sie dürfen die Dokumente nicht für öffentliche oder kommerzielle
Zwecke vervielfältigen, öffentlich ausstellen, öffentlich zugänglich
machen, vertreiben oder anderweitig nutzen.
Sofern die Verfasser die Dokumente unter Open-Content-Lizenzen
(insbesondere CC-Lizenzen) zur Verfügung gestellt haben sollten,
gelten abweichend von diesen Nutzungsbedingungen die in der dort
genannten Lizenz gewährten Nutzungsrechte.
Terms of use:
Documents in EconStor may be saved and copied for your personal
and scholarly purposes.
You are not to copy documents for public or commercial purposes, to
exhibit the documents publicly, to make them publicly available on the
internet, or to distribute or otherwise use the documents in public.
If the documents have been made available under an Open Content
Licence (especially Creative Commons Licences), you may exercise
further usage rights as specified in the indicated licence.
https://creativecommons.org/licenses/by/4.0/
S.Afr.J.Bus.Manage.2004,35(4) 27
The relationships between service quality, customer satisfaction and
buying intentions in the private hospital industry
C. Boshoff* and B. Gray
Department of Business Management, University of Port Elizabeth
PO Box 1600, Port Elizabeth 6000, Republic of South Africa
Received August 2004
The objective of this study was to investigate whether superior service quality and superior transaction-
specific customer satisfaction will enhance loyalty (as measured by purchasing intentions) among patients in
the private health care industry. The research design allowed an assessment of the relative impact of
individual dimensions of service quality and transaction-specific customer satisfaction on two dependent
variables, namely loyalty (as measured by intentions to repurchase) and customer satisfaction, the latter
measured as ‘overall’ or cumulative satisfaction.
The results reveal that the service quality dimensions Empathy of nursing staff and Assurance impact
positively on both Loyalty and Cumulative satisfaction.
The customer satisfaction dimensions Satisfaction with meals, Satisfaction with the nursing staff and
Satisfaction with fees all impact positively on both Loyalty and Cumulative satisfaction
*To whom all correspondence should be addressed.
Introduction
Every marketing textbook exhorts marketers to differentiate
themselves from competitors and competing brands (Lamb,
Hair, McDaniel, Boshoff & Terblanche, 2004). The
suggested differentiating variables range from branding to
convenience to price differentiation. However, many if not
most firms operate in markets where competing firms have
very similar cost structures which make price competition
difficult.
As most of the differentiating variables suggested in the
literature are easily copied by competitors, many firms are
focusing their efforts on quality of customer service as a
means of differentiation. Providing quality that meets or
exceeds customer expectations has become a major source
of competitive advantage for many firms as it reduces price
elasticities and builds loyalty and customer retention
(Anderson & Fornell, 1994:242). Service quality has also
been shown to be an important driver of customer
satisfaction both from a theoretical viewpoint (Heskett,
Sasser & Schlesinger, 1997) and empirically substantiated in
a variety of industries (Anderson & Sullivan, 1993;
Churchill & Suprenant, 1982) including service industries
such as tourism (Green & Boshoff, 2003) and health care
(Woodside, Frey & Daly, 1989).
The empirical findings of studies investigating the
relationships between service quality, customer satisfaction
and their outcomes have found broad support (Loveman,
1998: 18-31; Anderson & Mittal, 2000) for the relationships
described in the Service-Profit Chain suggested by Heskett,
Sasser and Schlesinger (1997). These relationships have,
however, not been considered in the South African private
hospital industry. This study thus attempts to assess what
dimensions of both customer satisfaction and service quality
drive ‘overall satisfaction’ and loyalty in the South African
private hospital industry.
Service quality
The first attempt to describe and define service quality was
the paradigm suggested by Grönroos (1983) who
distinguished between technical quality (what is done) and
functional quality (how it is done). The early work of
Grönroos (1983) was later extended by Parasuraman,
Zeithaml and Berry (1985:42). They argued that to fully
understand service quality, the intangible, heterogeneous
and inseparable nature of services must be acknowledged
and that service quality can be defined as the consumer’s
overall impression of the relative inferiority/superiority of
the organisation and its services (Bitner & Hubbert, 1994) or
as the customer's assessment of the overall excellence or
superiority of the service (Zeithaml, 1988). In these terms
service quality means conforming to customer expectations
(Lewis & Booms, 1983) and implies, from a consumer
perspective, the comparison of customer expectations with
customer perceptions of actual service performance
(Parasuraman et al., 1985).
28 S.Afr.J.Bus.Manage.2004,35(4)
The concept of customer satisfaction
In the service environment, one customer satisfaction-
related debate is of particular importance, namely whether
customer satisfaction is an outcome or a process (Yi,
1991:69). To date there seems to be two schools of thought.
Churchill and Suprenant (1982) and Oliver (1989), on the
one hand, view customer satisfaction as an outcome
resulting from the consumption experience. To Hunt
(1977:455), on the other hand, satisfaction is not the
pleasure of the experience, it is the evaluation rendered that
the experience was at least as good as it was supposed to be.
The ‘satisfaction as a process’ school stresses that
satisfaction or dissatisfaction is not inherent in the product
but, instead, is the individual’s perceptions of that product’s
attributes as they relate to that individual. Thus, satisfaction
is idiosyncratic and, as a construct, is formed by the
interaction of perceptual interpretations of the service and
consumer expectations of that service. As a consequence,
different consumers will have varying levels of satisfaction
for an experience which is essentially the same.
Although both schools of thought (satisfaction as an
outcome and as a process) have been widely recognised, the
process-oriented approach seems more appropriate in the
service environment given that consumption is an
experience and consists of collective perceptual, evaluative
and psychological processes that combine to generate
consumer satisfaction. In addition, the nature of services
(eg, intangibility) and the peculiarities of marketing services
(eg, inseparability) necessitate a distinction between
‘overall’ or cumulative satisfaction and satisfaction with a
specific service encounter (transaction-specific satisfaction),
an important distinction which is often ignored (Bitner &
Hubbert, 1994; Voss & Parasuraman, 1995).
From an encounter-specific perspective, satisfaction is
viewed as a post-choice evaluative judgement of a specific
purchase occasion. Most behavioural research can be
interpreted as focusing on this conceptualisation. This
perspective is insufficient to explain customer satisfaction
for, as Bitner and Hubbert (1994) point out, the evaluation
of each encounter will not necessarily correlate with the
customer’s overall satisfaction with the firm or perceptions
of the firm’s quality. Over time, however, it is likely that
multiple service encounters will lead to an overall level of
satisfaction.
More recently, research has focused on satisfaction at a
more general or organisational level. From this brand-
specific perspective, satisfaction is an overall evaluation
based on many transient experiences with a good or service
over time and, as such, satisfaction can also be thought of as
an ongoing evaluation of a firm’s ability to deliver the
benefits a customer is seeking. Bitner and Hubbert (1994)
point out that overall satisfaction is likely to be
multidimensional and based on all encounters and
experiences with that particular service firm. These multiple
encounters may include several interactions with one person
as well as experiences with multiple contact persons in the
same firm (Oliva, Oliver & MacMillan, 1992). Thus,
transactional satisfaction can be considered a contributor
and subsequent modifier to a less dynamic attitude of
satisfaction at an organisational level, while overall
satisfaction can be considered as the customer’s global
evaluation of the product/service offering.
No matter how we perceive customer satisfaction, however,
there can be no doubt that it is the key to profitability
(maybe not the only one, admittedly) over the long term
(Oliver, 1997: 10) also in a hospital environment (Raju &
Lonial, 2001:140-154).
Loyalty
Some commentators, somewhat cynically, suggest that there
are just two types of consumers, namely those who are
intrinsically loyal to a brand or store and those potential
switchers who, on every purchase occasion again choose
between competing offerings (Colombo & Morrison, 1989).
Keeping customers loyal is not easy, but its importance can
hardly be overstated. In fact, consumer loyalty has been
described as the marketplace currency for the twenty-first
century (Singh & Sirdeshmukh, 2000).
Customer loyalty has been defined in various ways, from a
probability of repurchase to proportion of purchase (Sivadas
& Baker-Prewitt, 2000). At a general level, customer loyalty
is a positive propensity toward a store or brand (East,
Hammond, Harris & Lomax, 2000). A critical review of the
many definitions of loyalty suggests that loyalty is both a
cognitive construct (attitude) and a shopping behaviour
(Dick & Basu, 1994; Mellens, Dekimpe & Steenkamp,
1996).
Whilst loyalty in a health care and particularly a hospital
environment differs from brand or store loyalty (it is often
the physician who makes the choice or strongly influences
the choice of a hospital) there can be no doubt that the same
benefits of loyalty accrue to a hospital as would to a retailer
or bank, for instance.
No matter what the industry under discussion, loyal
customers are a competitive asset to any business
organisation (Dekimpe, Steenkamp, Mellens & Vanden
Abeele, 1997) as customer loyalty serves as a barrier to
competitive entry (Aaker, 1991) and thus, by implication, is
also a key determinant in predicting market share (Baldinger
& Rubinson, 1997; Jacoby & Chestnut, 1978) and
profitability (Reichheld, 1996).
The antecedents of loyalty
A review of the literature reveals numerous studies that have
reported a positive relationship between satisfaction and
measures of repurchase intentions (Bloemer & De Ruyter,
1998; Loveman, 1998; Jones, Mothersbaugh, & Beatty,
2000) and between positive service quality perceptions and
loyalty.
The South African health care sector
A fairly ‘pure’ service sector such as the health care sector
can be quite varied, especially with the inclusion of the
many ancillary services. Traditionally, the South African
health care sector has consisted of two industries, namely,
S.Afr.J.Bus.Manage.2004,35(4) 29
private hospitals and public hospitals. Recently, a major
development in the hospital environment has been the
emergence of public/private partnership hospitals (Wilson,
2002:90). Public hospitals are by far the larger industry. In
contrast, private hospitals, the majority of which are
Hospital Association of South Africa (HASA) members,
make up approximately one third of South Africa’ s
hospitals.
The private hospital industry
There are about 178 private hospitals in South Africa. Three
groups, namely Netcare, Afrox Health care Limited and
Medi-Clinic currently dominate South Africa’s private
hospital industry. The independents and smaller groups
comprise Clinix, Community Health, Curamed, Joint
Medical Holdings, Melomed and the Protector Group. The
three major players collectively own 80% of hospital beds in
the private health care industry (Bhoola, 2002:55).
The South African private health care market is an
increasingly competitive environment. Private hospitals in
particular compete aggressively to attract patients. As in any
other competitive environment competing hospitals have to
differentiate themselves in the minds of consumers and ensure
that their patients leave satisfied so as to ensure that they return
again and in this way ensure the hospital’s long-term survival.
Objectives
The objective of the study was to investigate whether, if a
private hospital can differentiate itself by means of superior
service quality and superior transaction-specific customer
satisfaction, it will be able to enhance loyalty (as measured
by purchasing intentions) among its patients. More
specifically, an attempt was made to assess which
dimensions of service quality and transaction-specific
customer satisfaction exert the strongest influence on two
dependent variables, namely loyalty (as measured by
intentions to repurchase) and customer satisfaction, the latter
measured as ‘overall’ or cumulative satisfaction (Johnson,
Anderson & Fornell, 1995).
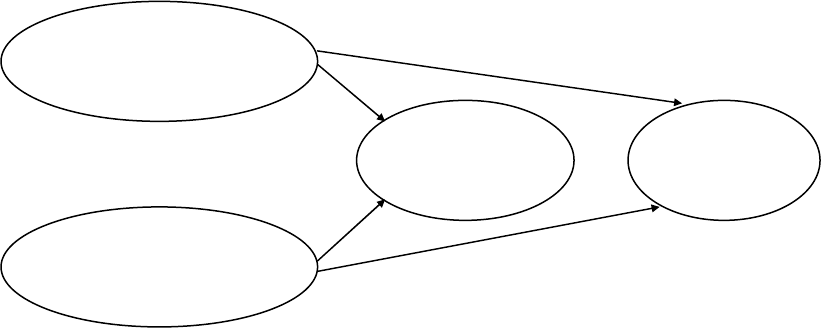
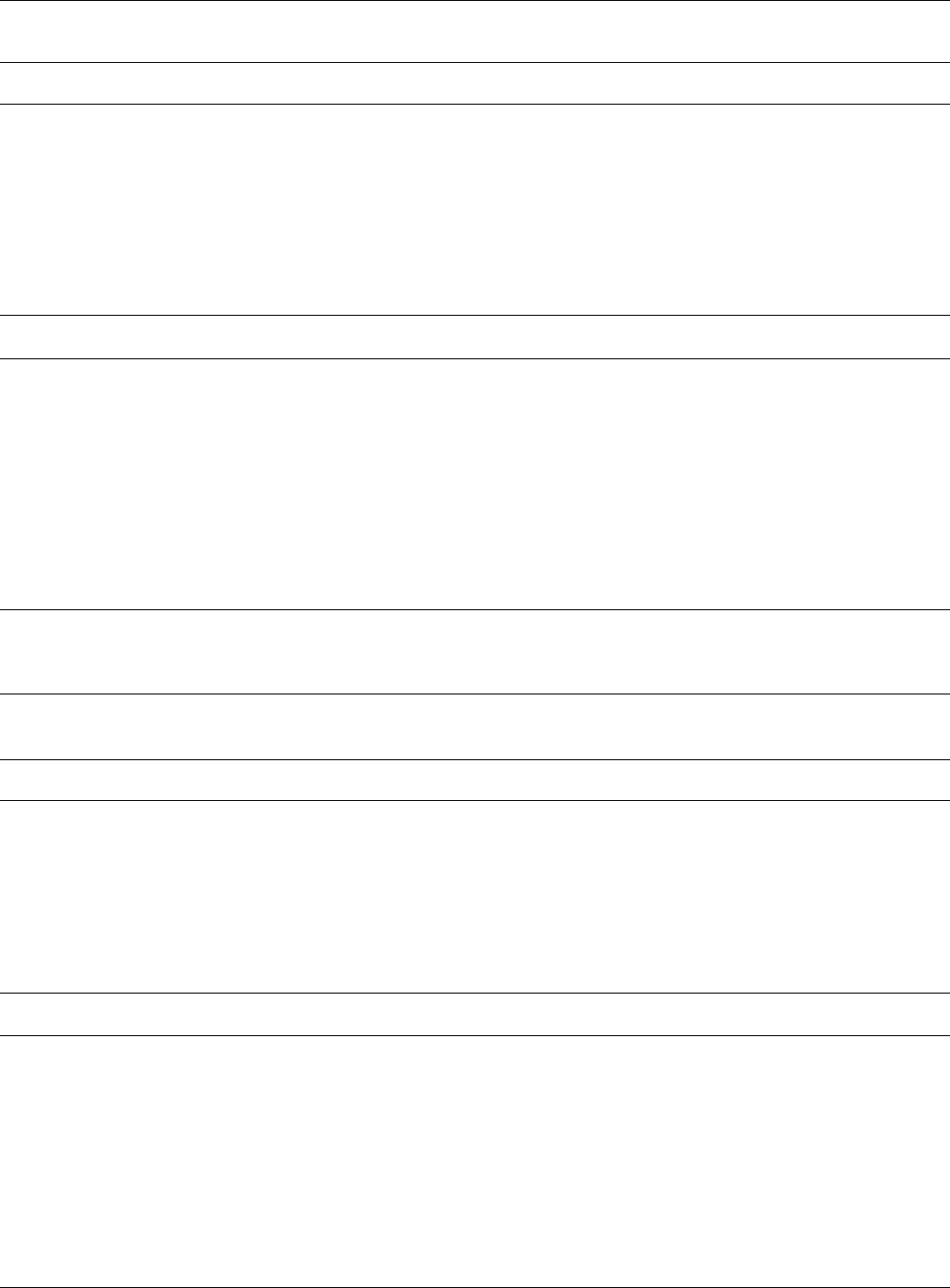
Figure 1 suggests that meeting consumer needs at the
attribute level will enhance cumulative customer satisfaction
which will in turn enhance loyalty/buying intentions and by
implication profitability as predicted by the Satisfaction-
Profit chain (Anderson & Mittal 2000:107-120).
Figure 1: The hypothesised relationships
Hypotheses
To assess the theoretical model depicted in Figure 1 the
following hypotheses were considered:
H
1
There is a positive relationship between perceived
service quality at the dimensional level and loyalty as
measured by buying intentions
H
2
There is a positive relationship between perceived
service quality at the dimensional level and cumulative
customer satisfaction
H
3
There is a positive relationship between customer
satisfaction at the dimensional level and loyalty as
measured by buying intentions
H
4
There is a positive relationship between customer
satisfaction at the dimensional level and cumulative
customer satisfaction
The research design
The measures
The best-known method of operationalising service quality
is the Gaps Model/SERVQUAL approach suggested by
Parasuraman, Zeithaml and Berry (1988). It is based on the
‘expectancy disconfirmation’ paradigm and measures
service quality perceptions (as opposed to so-called
‘objective’ quality) by comparing customer expectations
with the service performance.
During the initial operationalisation, model development
and scale development processes Parasuraman, Zeithaml
and Berry (1985) suggested that service quality consists of
10 dimensions, namely tangibles, reliability, responsiveness,
competence, courtesy, credibility, security, access,
communication and understanding the customer. This was
H
3
H
4
H
2
H
1
Perceived service
quality – dimensional level
Customer satisfaction -
dimensional level
Cumulative
customer
satisfaction
Loyalty –
buying
intentions
30 S.Afr.J.Bus.Manage.2004,35(4)
later reduced to just five dimensions, namely reliability,
assurance, responsiveness, empathy and tangibles.
To overcome at least some of the problems associated with
the use of SERVQUAL (Cronin & Taylor, 1992) service
quality was measured along the original 10 dimensions as
service quality is a stronger predictor of customer
satisfaction (Green & Boshoff, 2003) than the later 5-factor
configuration.
The SERVQUAL instrument has been subjected to a fair
amount of criticism for its poor validity. Such criticisms
include paradigmatic problems, questions about its
dimensionality and particularly its poor predictive validity
(Buttle, 1995). The problem is that at this moment there is
no credible alternative to SERVQUAL to measure service
quality. The original version of SERVQUAL, which
measures ten instead of five dimensions, was utilised in this
study (Zeithaml, Parasuraman & Berry, 1990:21-22) to
measure service quality.
Customer satisfaction with the actual hospital experience (at
the dimensional level) was measured with 53 statements
based on a thorough literature review (Woodside et al.,
1989; Jun, Peterson & Zsidisin, 1998; Reidenbach &
Sandifer-Smallwood, 1990), as well as on the exploratory
study that preceded the empirical survey. Cumulative (or
overall) satisfaction, a global assessment as opposed to a
dimensional assessment, was used as dependent variable as
it has been shown to be a better predictor of loyalty (Olsen
& Johnson, 2003:194). Cumulative satisfaction was
measured with the following three semantic differentially-
scaled items:
Overall, how satisfied were you with your stay at
….? (satisfied ´ dissatisfied)
How would you rate the overall standard of service
at …? (excellent ´ poor)
Did you comment on any aspect of your hospital
stay to any hospital staff member (praised ´
complained)
Because one cannot refer to loyalty in the private hospital
industry in the same manner as say, in a retail context (due to
the way the buying decision is made), buying intentions were
used as a surrogate measure of loyalty. Buying intentions have
successfully been used as a surrogate for loyalty in a service
environment before (Shaw-Ching, Furrer & Sudharshan,
2001). The dependent variable in this study was thus measured
using the following five items:
I would not mind returning to …. again in the
future
I would recommend this hospital to family and
friends
In an emergency this is the hospital I would like to
be admitted to …
I regard myself as a ‘loyal’ customer of …
I would definitely return to this hospital in the
future if necessary
All items were linked to a 7-point Likert scale ranging from
Strongly Agree (7) to Strongly Disagree (1).
The sample
The sampling procedure can be described as a combination of
convenience and random sampling. The hospitals that
participated in this study were selected on a convenience basis.
Questionnaires were distributed on a random basis to patients
who booked into four hospitals belonging to one private
hospital group. One hospital in Cape Town, Port Elizabeth,
Durban and two in Johannesburg participated in the study. To
qualify to participate in the study respondents had to be over
the age of 20 years; had to be there to undergo an operation
(anaesthetic included); and had to have at least one overnight
stay in a hospital ward.
In total 3 800 questionnaires were distributed of which 425
were returned and 323 (or 11,2%) could be statistically
analysed.
The questionnaire was a self-administered questionnaire. It
was accompanied by a covering letter and information on an
incentive to complete the questionnaire, as well as a reply-
paid envelope. The questionnaires could be handed in before
patients left the hospital or else mailed back once they had
returned home.
Data analyses
The data were analysed in three phases. During the first
phase the discriminant validity of the instruments used to
measure cumulative customer satisfaction and
loyalty/willingness to re-purchase was subjected to an
exploratory factor analysis. Once a clear factor structure
emerged, the internal reliability of each factor was assessed
using Cronbach’s Alpha. The factors that emerged after the
exploratory factor analysis phase were then used as
independent variables in four subsequent multiple regression
analyses to assess the relationships predicted by the four
hypotheses and graphically depicted in Figure 1.
The empirical results
Discriminant validity
To assess the discriminant validity of the instruments used
to measure both service quality and customer satisfaction,
the remaining items were subjected to an exploratory factor
analysis using the computer programme BMDP4M (Frane,
Jennrich & Sampson, 1990) by specifying a Maximum
Likelihood and a Direct Quartimin oblique rotation
(Jennrich & Sampson, 1966) of the original factor matrix.
A variety of different exploratory factor analysis solutions
were considered. The results revealed, however, that neither
the ten dimensions nor the five dimensions of service quality
proposed by Parasuraman et al., (1988), could be replicated.
The most interpretable factor structure was the one shown in
Table 1. A number of items did not demonstrate sufficient
discriminant validity by either cross-loading or not loading
to a significant extent and were then deleted. Table 1 shows
that the service quality items used from the initial
SERVQUAL loaded on seven distinct factors, namely
Communication (measured by three items), Credibility
(measured by four items), Tangibles (measured by five
S.Afr.J.Bus.Manage.2004,35(4) 31
items), Understanding (measured by six items),
Responsiveness (measured by four items), Security
(measured by two items) and Doctor’s responsiveness
(measured by two items).
These dimensions were operationalised as follows:
Communication the patient receiving
information about his condition,
treatment, procedures to be
conducted and post-discharge
treatment/care
Tangibles perceptions of the cleanliness of
the hospital in general and the
wards in particular, the neatness
of the buildings, the décor in the
wards and the appearance of the
nursing staff
Empathy of nursing staff the responsiveness of the
nursing staff, their
understanding, the adequacy
and individualisation of
attention, efficiency and a
warm/caring attitude
Assurance hospital caring about its
patients, the hospital’s
reputation, patients’ confidence
in the hospital and feeling safe
there
Responsiveness of
administrative staff speedy admission, efficient in
dealing with problems, sincerity
in solving problems, responsive
to requests
Security both inside and outside the
hospital
Physician responsiveness physicians attending to the
needs of patients and being
punctual in doing ward rounds
The items used to measure customer satisfaction were also
subjected to an exploratory factor analysis. The most
interpretable factor structure is the one reported in Table 2.
It shows customer satisfaction in a hospital consists of 7
dimensions, namely Satisfaction with meals (measured by
six items), Satisfaction with fees (measured by four items),
Satisfaction with the nursing staff (measured by four items),
Satisfaction with the admission process (measured by three
items), Satisfaction with the theatre experience (measured
by four items), Satisfaction with the TV service in the wards
(measured by two items) and Satisfaction with the ward
arrival (measured by two items).
The underlying dimensions of customer satisfaction were
operationalised as:
Meals being tasty, nutritious,
attractively presented and at
correct temperatures and
adequate variety
Fees that are reasonable, worth the
money, value for money and not
expensive
Nursing staff that are cheerful, responsive,
kind/caring and adequately
skilled
Admission courteous/helpful, prepared to
listen, prompt admission
Theatre experience receiving pre-med in time,
proper preparation for
operation, easing of fears,
explanation by anaesthetist
TV service in ward access to a TV that is
functioning properly
Ward arrival being told what to do and where
ward facilities are
Internal reliability
The next phase of the data analysis was to assess the internal
reliability of the instrument used to test the variables in the
theoretical model depicted in Figure 1. This was done by
calculating Cronbach Alpha coefficients using the computer
programme SAS (SAS Institute, 1990).
Tables 1 and 2 show that all of the instruments used returned
initial Cronbach Alpha coefficients above the 0.7 threshold
recommended by Nunnally (1978) and Peterson (1994).
Tables 1 and 2 thus confirm the reliability, the discriminant
and the construct validity of the instruments used to measure
the independent variables used in the subsequent multiple
regression analyses.
The regression analyses results
Table 3 shows that the service quality dimensions Empathy
of nursing staff (p < 0,001), Assurance (p < 0,001) and
Tangibles (p < 0,01) impact positively on Loyalty as
hypothesised. The impact of Security (p < 0,05) on Loyalty
is, however, negative. Hypothesis 1 is thus accepted in terms
of these four dimensions but rejected in respect of
Communication, Responsiveness and Physician
responsiveness.
32 S.Afr.J.Bus.Manage.2004,35(4)
Table 1: Exploratory factor analysis results rix for service quality items
Service Quality Dimensions
Factor 1 Factor 2 Factor 3 Factor 4 Factor 5 Factor 6 Factor 7
Commu-
nication
Tangibles Empathy
of
nursing
staff
Assurance Respons-
iveness
Security Physician
responsive-
ness
Patients assured of receiving adequate information about their
condition
0,945
Patients assured of receiving adequate information about their
treatment
0,890
Procedures thoroughly explained to patients 0,745
Discharge care thoroughly explained 0,546
Spotlessly clean wards at ___ 0,866
___ is a clean hospital 0,801
___ maintains a neat appearance of buildings 0,602
Tastefully decorated wards 0,552
Nursing staff look professional and neat in their uniforms 0,522
Service at ___ is excellent overall 0,444
Nurses never too busy to respond to patients’ needs 0,699
Nurses show understanding toward patients’ feelings of discomfort 0,644
Patients do not feel neglected by nursing staff 0,610
Patients are given plenty of individual attention 0,607
Nursing staff efficient at dealing with patients’ problems 0,421
Nurses show understanding when patients feel low 0,490
Nurses treat patients with a warm and caring attitude 0,493
___ cares about its patients 0,815
Patients feel safe at ___ hospital 0,796
___ has an excellent reputation 0,701
Patients can feel confident in treatment to be received 0,630
Administrative staff efficient at dealing with patients’
queries/problems
0,827
Admission handled quickly and efficiently by administrative staff 0,696
Administrative staff sincerely interested in solving patients’
problems
0,637
Administrative staff never too busy to respond to patients’ requests 0,630
Adequate security provided inside hospital 0,788
Adequate security provided outside hospital 0,754
Doctors are punctual when conducting ward rounds 0,723
Doctors can be counted on to attend to their patients’ needs 0,540
Eigen values: 15,45 1,74 1,47 1,33 1,07 0,90 0,89
Cronbach’s alpha: 0,92 0,88 0,95 0,95 0,87 0,82 0,77
Table 2: Factor matrix for customer satisfaction items
Customer Satisfaction Dimensions
Factor 1 Factor 2 Factor 3 Factor 4 Factor 5 Factor 6
Factor7
Meals Fees Nursing
Staff
Admission Theatre TV’s in
Wards
Ward
Arrival
Meals were tasty 0,987
Meals were nutritious 0,903
Meals were attractively presented 0,899
Overall, patient enjoyed the food while at ___ 0,876
Meals always served at correct temperature 0,715
Meals were served in a variety of ways 0,640
Fees at ___ are reasonable 0,880
Considering fees charged, stay worth the money 0,779
A stay at ___ is good value for money 0,773
___’s fees are not expensive 0,618
Nursing staff were always cheerful 0,888
Nursing staff responded promptly to patient’s needs 0,839
Nursing staff kind and caring throughout patient’s stay 0,706
Nursing staff were skilled in administering procedures 0,583
Administrative staff courteous and helpful at admissions counter 0,825
Administrative staff willing to listen to patient’s concerns 0,675
Patient’s admittance procedure carried out promptly 0,634
Pre-med (for surgery) was administered at correct time 0,824
Preparation for surgery carried out efficiently 0,569
Nursing staff eased patient’s fears about the surgery 0,517
Anaesthetist came to explain his role during surgery 0,403
Television sets functioned properly 0,993
Television set in the ward 0,671
Upon arrival in ward, nursing staff told patient what to do next
0,561
After arrival in ward, patient shown ablution/ward facilities
0,471
Eigen values: 9,76 2,91 1,69 1,44 1,28 1,20
0,84
Cronbach’s alpha: 0,94 0,89 0,91 0,79 0,77 0,80
0,77
S.Afr.J.Bus.Manage.2004,35(4) 33
Table 3 thus shows that the more patients perceive the
nursing staff as empathetic, feel assured and safe in the
hospital, and evaluate the physical environment (Tangibles)
positively, the more likely they are to remain loyal to the
hospital. In the case of Security, however, the relationship is
negative. In other words, too much security will reduce
Loyalty.
Table 3 reveals that the modelled independent variables
(service quality dimensions) explain 58,5% of the variation
in the dependent variable (Loyalty).
According to Table 4 only two service quality dimensions
namely Empathy of nursing staff (p < 0,001) and Assurance
(p < 0,001), impact positively on Cumulative satisfaction as
suggested by hypothesis 2. Hypothesis 2 is thus accepted in
terms of Empathy of nursing staff and Assurance but
rejected in respect of Communication, Tangibles,
Responsiveness, Security and Physician responsiveness.
Table 4 reveals that the modelled independent variables
(service quality dimensions) explain 60,3% of the variation
in the dependent variable (Loyalty).
When individual dimensions of customer satisfaction are
regressed on Loyalty, Table 5 shows that Satisfaction with
meals (p < 0,001), Satisfaction with the nursing staff (p <
0,001), Satisfaction with fees (p < 0,01) and Satisfaction
with the television service (p < 0,01) all impact positively on
Loyalty. Hypothesis H3 is thus accepted in terms of these
four dimensions but rejected in terms of Satisfaction with
admission, Satisfaction with ward arrival and Satisfaction
with the Theatre experience (p > 0,05).
Table 5 also shows that the strongest predictor of
Cumulative satisfaction is Satisfaction with the nursing staff
(estimate 0,386) and that the six dimensions of Cumulative
satisfaction included in the regression model explain 68,3%
of the variation in the dependent variable (Loyalty).
To assess the last hypothesis the impact of the individual
customer satisfaction dimensions on Cumulative satisfaction
(an “overall” assessment) was assessed. Table 6 shows that
Satisfaction with nursing staff (p < 0,001), Satisfaction with
fees (p < 0,001) and Satisfaction with meals (p < 0,01), all
exert a positive influence on Cumulative satisfaction as
suggested by H1 which is thus accepted. However, the
hypothesis is rejected in respect of Satisfaction with
administration, Satisfaction with Arrival, Satisfaction with
the theatre experience and Satisfaction with the TV service.
Table 6 also shows that Satisfaction with the nursing staff is
the strongest predictor of Cumulative satisfaction and that
66,0% of the variation in the dependent variable (Loyalty) is
explained by the seven independent variables (satisfaction
dimensions).
Managerial implications
If a private hospital sets itself the goal of enhancing loyalty
of its patients, it is clear from Table 3 that service quality
efforts will have to be focused on the Empathetic behaviour
of its nursing staff and conveying a sense of Assurance.
Nursing training will thus have to move beyond normal
nursing skills, competencies and efficiency to also
emphasise ‘softer’ skills such the responsiveness of the
nursing staff, their understanding of patients’ concerns and
fears, providing individualised attention and developing the
ability to demonstrate a warm/caring attitude towards
patients. To convey a sense of Assurance, on the other hand,
the hospital will have to cultivate a perception that will be
based on more than just interaction with the nursing staff.
During the whole hospitalisation experience and at each
‘contact point’ all employees should demonstrate that they
care about its patients, are careful in protecting and
enhancing the hospital’s reputation, do everything to gain
the patients’ confidence in the hospital and ensure that
patients feel safe during their hospitalisation. Table 4 shows
that careful management of the Empathy of the nursing staff
and of feelings of Assurance will not only enhance patient
Loyalty but will also enhance patients’ ratings of their
overall or cumulative satisfaction.
Another dimension that impacts on patient Loyalty (which can
be described as a ‘hard issue’) is Tangibles. Tangibles are a
service quality dimension that has proved relatively
unimportant in many service quality studies (Zeithaml et al.,
1990:29). It is obviously different in the hospital environment.
Perceptions of the cleanliness of the hospital in general and the
wards in particular, the neatness of the buildings, the décor in
the wards and the appearance of the nursing staff will all
influence whether a patient will return to a hospital or not.
Tangibles are typically the easiest service quality dimension to
manage and manipulate as they do not involve people.
The fourth service quality dimension to impact on Loyalty is
Security (see Table 4). In other words, it appears as if a too
strong security presence (too many and/or heavily armed
security guards, inappropriate security fencing etc) can
actually raise concerns and scare-off patients, and will
reduce their intentions to again patronise the hospital.
Security arrangements must thus be implemented very
discreetly and care taken not to overdo the installation of
visible security measures.
Perceptions of loyalty can also be enhanced by ensuring
satisfaction with transaction-specific dimensions of the
service rendered. Table 5 shows that customer satisfaction
with the meals provided, satisfaction with the nursing staff,
satisfaction with the fees paid and satisfaction with the TV
service in the wards will encourage patients to return to the
hospital in the future. In other words, tasty, attractive,
nutritious meals combined with variety will make patients
want to come back. Table 5 underlines the critically
important role that the nursing staff play in all facets of
patients’ evaluation. If patients experience the nursing staff
as cheerful, kind, caring, courteous as well as highly skilled
and prompt, they are significantly more likely to return to
the same hospital should the need arise.
34 S.Afr.J.Bus.Manage.2004,35(4)
Table 3: Multiple regression results: Impact of service quality dimensions on loyalty
Dependent Variable: LOYALTY (Buying intentions or willingness to re-purchase)
Sum of Mean
Source DF Squares Square F value Pr > F
Model 7 2013,39 287,63 63,56 0,0001
Error 315 1425,56 4,53
Corrected Total 322 3438,95
R
2
C.V. Root MSE Loyalty Mean
58,5% 11,92 2,13 17,84
Exceedance Std Error
Parameter Estimate T-value probability of estimate
INTERCEPT 2,024 2,04 0,0418 0,990
COMMUNICATION 0,048 1,16 0,2478 0,041
EMPATHY: NURSING STAFF 0,160 5,81 0,0001*** 0,028
TANGIBLES 0,126 2,97 0,0032** 0,043
ASSURANCE 0,227 4,01 0,0001*** 0,057
RESPONSIVENESS: ADMIN 0,026 0,61 0,5440 0,043
SECURITY -0,147 -2,15 0,0323* 0,068
RESPONSIVENESS: PHYSICIAN -0,003 -0,04 0,9669 0,076
---------------------
*** = p < ,001
** = p < 0,01
* = p < 0,05
Table 4: Multiple regression results: Impact of service quality dimensions on cumulative satisfaction
Dependent Variable: CUMULATIVE SATISFACTION
Sum of Mean
Source DF Squares Square F value Pr > F
Model 7 6797,42 971,06 68,46 0,0001
Error 315 4467,76 4,18
Corrected Total 322 11265,18
R
2
C.V. Root MSE CUM SAT Mean
60,3% 12,37 3,77 30,43
Exceedance Std Error
Parameter Estimate T-value probability of estimate
INTERCEPT 1,512 0,86 0,3890 1,753
COMMUNICATION -0,082 -1,12 0,2651 0,073
EMPATHY: NURSING STAFF 0,274 5,64 0,0001*** 0,049
TANGIBLES 0,096 1,28 0,2028 0,075
ASSURANCE 0,653 6,51 0,0001*** 0,100
RESPONSIVENESS: ADMIN 0,050 0,66 0,5110 0,076
SECURITY -0,050 -0,41 0,6806 0,121
RESPONSIVENESS: PHYSICIAN 0,028 0,21 0,8323 0,134
---------------------
*** = p < ,001
** = p < 0,01
* = p < 0,05
S.Afr.J.Bus.Manage.2004,35(4) 35
Table 5: Multiple regression results: Impact of satisfaction dimensions on loyalty
Dependent Variable: LOYALTY (Willingness to re-purchase)
Sum of Mean
Source DF Squares Square F value Pr > F
Model 7 2348,97 335,57 96,98 0,0001
Error 315 1089,98 3,460
Corrected Total 322 3438,95
R
2
C.V. Root MSE LOYALTY Mean
68.3% 10,43 1,86 17,84
Exceedance Std Error
Parameter Estimate T-value probability of estimate
INTERCEPT 2,0622 2,46 0,0143 0,837
MEALS 0,066 4,50 0,0001*** 0,015
NURSING STAFF 0,386 11,99 0,0001*** 0,032
FEES 0,080 2,77 0,0060** 0,029
ADMISSION 0,025 0,55 0,5852 0,046
WARD ARRIVAL 0,028 1,02 0,3067 0,027
THEATRE 0,020 0,63 0,5260 0,032
TV 0,129 2,67 0,0079** 0,048
---------------------
*** = p < ,001
** = p < 0,01
* = p < 0,05
Table 6: Multiple regression results: Impact of satisfaction dimensions on cumulative satisfaction
Dependent Variable: CUMULATIVE SATISFACTION
Sum of Mean
Source DF Squares Square F value Pr > F
Model 7 7439,27 1062,75 87,50 0,0001
Error 315 3825,92 12,15
Corrected Total 322 11265,18
R
2
C.V. Root MSE CUM SAT Mean
66.0% 11,45 3,485 30,430341
Exceedance Std Error
Parameter Estimate T-value probability of estimate
INTERCEPT 2,763 1,76 0,0790 1,568
MEALS 0,083 3,03 0,0026** 0,027
NURSING STAFF 0,664 11,00 0,0001*** 0,060
FEES 0,309 5,71 0,0001*** 0,054
ADMISSION -0,021 -0,24 0,8111 0,086
WARD ARRIVAL 0,0909 1,81 0,0715 0,050
THEATRE 0,0504 0,85 0,3936 0,059
TV 0,0714 0,79 0,4286 0,090
---------------------
*** = p < .001
** = p < 0.01
* = p < 0.05
36 S.Afr.J.Bus.Manage.2004,35(4)
According to Table 5 patients are also more likely to return
to a hospital (loyalty) if they perceive the fees that they are
charged as fair, reasonable and good value for the money
paid (fees), and if, when they have access to a TV service in
the wards, this service functions effectively. Hospital
managers must thus ensure that patients are not overcharged,
that they receive an itemised account and even, when
necessary, provide a justification or an explanation for
exceptional charges. Furthermore, it appears as if patients
regard a functional TV service as ‘a given’ and care must be
taken to ensure that the service is always functional and that
a back-up TV or repair staff are available to ensure an
uninterrupted service.
Table 6 confirms that the same transaction-specific
dimensions also impact on Cumulative satisfaction, except
for the TV service. In other words, patients who report high
levels of satisfaction with the meals provided, satisfaction
with the nursing staff and satisfaction with the fees paid,
will besides remaining Loyal to the hospital, also report high
levels of satisfaction with the service encountered.
References
Aaker, D.A. 1991. ‘Measuring brand equity across products
and markets’, California Management Review, 38(2):102-
120.
Anderson, E.W. & Fornell, C. 1994. ‘A customer
satisfaction research prospectus’. In Rust, R.T. & Oliver,
R.L. (Eds.). Service quality: New directions in theory and
practice. Thousand Oaks, California: Sage Publications, pp.
241-268.
Anderson, E.W. & Mittal, V. 2000. ‘Strengthening the
satisfaction-profit chain’, Journal of Service Research,
3(2):107-120.
Anderson, E.W. & Sullivan, M.W. 1993. ‘The antecedents
and consequences of customer satisfaction for firms’,
Marketing Science, 12(2):25-143.
Baldinger, A.L. & Rubinson, J. 1997. ‘The jeopardy in
double jeopardy’, Journal of Advertising Research,
37(6):37-49.
Bhoola, R. 2002. Health Annals. Independent hospitals in
the private hospital industry. 11
th
Annual publication of the
Hospital Association of South Africa. Johannesburg: The
Hospital Association of South Africa (HASA).
Bitner, M.J. & Hubbert, A.R. 1994. ‘Encounter satisfaction
versus overall satisfaction versus quality: The customers
voice’. In Rust, R.T. & Oliver R.L. (Eds.). Service Quality:
New directions in theory and practice, Thousand Oaks,
California, Sage Publications, pp. 72-94,
Bloemer, J. & De Ruyter, K. 1998. ‘On the relationship
between store image, store satisfaction and store loyalty’,
European Journal of Marketing, 32(5/6): 499-513.
Buttle, F.A. 1995. ‘What future for SERVQUAL?’ In
Proceedings of the European Marketing Academy’s 24
th
Annual Conference, Paris, 16-19 May, pp.211-230.
Churchill, G.A. Jr. & Suprenant, C. 1982. ‘An investigation
into the determinants of customer satisfaction’, Journal of
Marketing Research, 19(4):491-504.
Colombo, R.A. & Morrison, D.G. 1989. ‘A brand switching
model with implications for marketing strategies’,
Marketing Science, 8(1):88-99.
Cronin, J.J. & Taylor, S.A. 1992. ‘Measuring service
quality: A re-examination and extention’, Journal of
Marketing, 56(3):55-68.
Dekimpe, M.G., Steenkamp, J.E.M., Mellens, M. & Van den
Abeele, P. 1997. ‘Decline and variability in brand loyalty’,
International Journal of Research in Marketing, 14(5):405-
420.
Dick, A.S., & Basu, K. 1994. ‘Customer loyalty: Towards
an integrated framework,’ Journal of the Academy of
Marketing Science, 22(2):99-113.
East, R., Hammond, K., Harris, P. & Lomax, W. 2000.
‘First-store loyalty and retention’, Journal of Marketing
Management:16, 307-325.
Frane, J., Jennrich, R.I., & Sampson, P.F. 1990. ‘P4M
Factor Analysis’. In Dixon, W.J. & Brown, M.B. (Eds.).
BMDP Statistical Software Manual, Vol 1. Berkeley:
University of California, Berkeley, pp. 311-337.
Green, S. & Boshoff, C. 2003. ‘An empirical assessment of
the relationships between service quality, satisfaction and
value: A tourism study,’ Management Dynamics, 11(3):1-
16.
Grönroos, C. 1983. ‘Innovative marketing strategies and
organization structures for service firms’. In Berry, L.L.,
Shostack, G.L. & Upah, G.D. (Eds.). Emerging perspectives
on services marketing. Chicago, Ill.: American Marketing
Association.
Heskett, J., Sasser, W. & Schlesinger, L. 1997. The service-
profit chain. New York: The Free Press.
Hunt, H.K. 1977. ‘CS/D - Overview and future research
directions’. In Hunt, H.K. (Ed.). Conceptualisation and
measurement of customer satisfaction and dissatisfaction.
Cambridge, MA: Marketing Science Institute, pp. 455-488.
Jacoby, J. & Chestnut, R.W. 1978. Brand loyalty
measurement and management. New York : Wiley.
Jennrich, R.I. & Sampson, P.F. 1966. ‘Rotation for simple
loadings’, Psychometrica, 31:313-323.
Jones, M.A., Mothersbaugh, D.L., & Beatty, S.E. 2000.
‘Switching barriers and repurchase intentions in services’,
Journal of Retailing, 76(2): 259–274.
S.Afr.J.Bus.Manage.2004,35(4) 37
Johnson, M.D. Anderson, E.W. & Fornell, C. 1995.
‘Rational and adaptive performance expectations in a
customer satisfaction framework’, Journal of Consumer
Research, 21:128-140.
Jun, M., Peterson, R.T. & Zsidisin, G.A. 1998. ‘The
identification and measurement of quality dimensions in
health care: Focus group interview results’, Health Care
Management Review, 23(4):81-96.
Lamb, C.W., Hair, J.F., McDaniel, C., Boshoff, C. &
Terblanche, N.S. 2004. Marketing. 2
nd
South African
Edition. Cape Town: Oxford University Press.
Lewis, R.C. & Booms, B.H. 1983. ‘The marketing aspects
of service quality’. In Berry, L.L., Shostack, G.L. & Upah,
G.D. (Eds.). Emerging perspectives on services marketing.
Chicago: American Marketing Association, pp. 99-107.
Loveman, G.W. 1998. ‘Employee satisfaction, customer
loyalty and financial performance: An empirical
examination of the service profit chain in retail banking’,
Journal of Service Research, 1(1):18-31.
Mellens, M., Dekimpe, M.G. & Steenkamp, J. E. M. 1996.
‘A review of brand-loyalty measures in marketing’,
Tijdschrift voor Economie en Management, 41(4): 507-533.
Nunnally, J. 1978. Psychometric theory. 2nd Edition. New
York: Mc Graw-Hill.
Oliva, T.A., Oliver, R.L. & MacMillan, I.C. 1992. ‘A
catastrophe model for developing service satisfaction
strategies’, Journal of Marketing, 56(2):83-95.
Oliver, R.L. 1997. Customer satisfaction: A behavioral
perspective on the consumer. New York: McGraw-Hill.
Oliver, R.L. 1989. ‘Processing of the satisfaction response
in consumption: A suggested framework for research
propositions’, Journal of Consumer Satisfaction,
Dissatisfaction and Complaining Behaviour, 2:1-16.
Olsen, L.L. & Johnson, M.D. 2003. ‘Service equity,
satisfaction and loyalty: From transaction-specific to
cumulative evaluations’, Journal of Service Research,
5(3):184 – 195.
Parasuraman, A., Zeithaml, V.A. & Berry, L.L. 1985. ‘A
conceptual model of service quality and its implications for
future research’, Journal of Marketing, 49(4): 41-50.
Parasuraman, A., Zeithaml, V.A. & Berry, L.L. 1988.
‘SERVQUAL: A multi-item scale for measuring consumer
perceptions of service quality’, Journal of Retailing,
64(1):12-40.
Peterson, R.A. 1994. ‘A meta-analysis of Cronbach’s
coefficient alpha’, Journal of Consumer Research,
21(3):381-391.
Raju, P.S. & Lonial, S.C. 2001. ‘The impact of quality
context and market orientation on organizational
performance in a services environment’, Journal of Service
Research, 4(2):140-154.
Reichheld, F.F. 1996. The loyalty effect – the hidden force
behind growth, profits and lasting value. Boston, MA:
Harvard Business School Press.
Reidenbach, R.E. & Sandifer-Smallwood, B. 1990.
‘Exploring perceptions of hospital operations by a modified
SERVQUAL approach’, Journal of Health Care Marketing,
10(4):47-55.
SAS Institute Inc. 1990. SAS Procedures. Release 6.03
Edition. Cary, North Carolina: SAS Institute.
Shaw-Ching, L.B., Furrer, O. & Sudharsan, D. 2001. ‘The
relationships between culture and behavioral intentions
toward services’, Journal of Service Research, 4(2): 118-
129.
Singh, J. & Sirdeshmukh, D. 2000. ‘Agency and trust
mechanisms in relational exchanges’, Journal of the
Academy of Marketing Science, 28(1):150-167.
Sivadas, E. & Baker-Prewitt, J.L. 2000. ‘An examination of
the relationship between service quality, customer
satisfaction, and store loyalty’, International Journal of
Retail & Distribution Management, 28(2):73-82.
Voss, G.B. & Parasuraman, A. 1995. Prepurchase
preference and postpurchase satisfaction in service
exchange. Working Paper, Marketing Science Institute,
Report Number 95-113, October.
Woodside, A.G., Frey, L.L. & Daly, R.T., 1989. ‘Linking
service quality, customer satisfaction, and behavioural
intention’, Journal of Health care Marketing, 9(4):5-17.
Wilson, S. 2002. Health Annals. A new dawn in African
health care facilities management. 11
th
Annual publication
of the Hospital Association of South Africa. Johannesburg:
The Hospital Association of South Africa (HASA).
Yi, Y. 1991. ‘A critical review of customer satisfaction’. In
Zeithaml, V.A. (Ed.). Review of marketing 1990. Chicago:
American Marketing Association, pp. 68-123.
Zeithaml, V.A. 1988. ‘Consumer perceptions of price,
quality, and value: A means-end model and synthesis of
evidence’, Journal of Marketing, 52 (3):2-22.
Zeithaml, V.A., Parasuraman, A. & Berry, L.L. 1990.
Delivering quality service. New York: The Free Press.
38 S.Afr.J.Bus.Manage.2004,35(4)
